Please Read All Descriptions, Indications and Warnings Before Use
DESCRIPTION
The pediatric device for induction of anesthesia (PeDIA) is an alternative to a face mask for the inhalation induction of anesthesia and is intended for the delivery of nitrous and/or anesthetic gases to children age three years and older. It is intended to be used prior to IV insertion, LMA/endotracheal intubation, and/or conversion to a standard mask induction.
Please Read All Descriptions, Indications and Warnings Before Use
Instructions for the anesthesia professionals:
Attach the universal connector of the PeDIA to the anesthesia breathing circuit as you would the anesthesia mask.
Turn the APL valve (pop-off) to minimum.
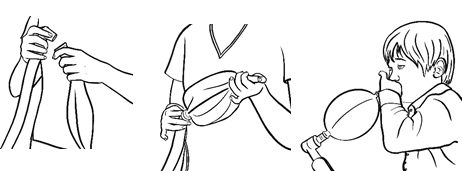
Obstruct the whistle/mouthpiece using your thumb/finger to trap gases inside balloon.
Turn up flows of oxygen and nitrous oxide sufficient to inflate the PeDIA.
Hand the child the inflated PeDIA Balloon.
Be sure the child seals their lips around the mouthpiece.
Be sure child inhales and exhales only through the mouth, not the nose.
As the child exhales and inhales, observe the system is working properly.
PIPs remain low
Balloon slightly inflates and deflates.
After 2-3 breaths, dial-in the volatile anesthetic of choice.*
When the child falls asleep or is too sleepy to hold a proper seal lips around whistle, take the PeDIA from the child and lay the child supine.
Detach PeDIA from the anesthesia circuit using a gentle pull.
Attach the anesthesia mask to the breathing circuit.**
Support patient respiration with mask-ventilation and continue induction/intubation.
Discard the PeDIA per facility protocol.
*Noncombustible anesthetic agents should be used with gas flows and anesthetic concentrations determined by the anesthesia provider.
**Before switching to a mask, the practitioner may elect to vent the gases into the circuit.
Instructions: Pediatric Device for Induction of Anesthesia Please read all instructions before use.
WARNINGS:
Warnings:
Consult instructions for use
Single use; disposable
Keep dry
Caution
No components of the PeDIA are made of latex
Disposables delivered are non-sterile
DO NOT send any portion of the device home with the child
DO NOT use if the device is damaged
DO NOT use if the packaging is damaged
DO NOT use with combustible volatile anesthetics
DO NOT sterilize the device
DO NOT reuse the device or share between patients
DO NOT separate the body of the device from the mouthpiece
DO NOT use with children who cannot or will not follow directions
Restricted to sale by or on the order of a physician
Manufacturer of Record
Date of manufactured unit
Catalog Number
Lot Number
Do not use if packaging is open or damaged
Do perform an anesthesia machine check per ASA guidelines to include the scavenger system
Do instruct the child on the proper use of the device
Do inspect the device for signs of damage
Do set and maintain the Adjustable Pressure Limiting Valve (APL or pop-off) to minimum
Discontinue use with signs of increased pressure within the PeDIA such as:
− A taut balloon or increase Peak Inspiratory Pressures (PIP).
− Any signs of patient distress
− The patient cannot or will not follow directions
https://pediallc.com/wp-content/uploads/2021/08/Blog-pic-1.jpg672896dianemillerhttps://pediallc.com/wp-content/uploads/2021/02/PeDIA_header_1.pngdianemiller2021-08-30 19:42:142025-06-26 19:29:08Instructions For Use PEDIA Anesthesia Balloons
A Child’s Experience During Induction of Anesthesia: Strangers Forcing A Plastic Mask Over Their Face.
It’s Time For A Change
In the 21st century, science and technology have launched medicine into territories once relegated to the areas of science fiction. Robotic assisted surgery and computer-aided navigation have granted vision and precision in the surgical field just as ultrasound imaging guidance has done for anesthesia. The video laryngoscope, like CoPilotVL, proved itself invaluable for difficult intubation and is on the fast-track to becoming a standard of care. Nonetheless, while some areas of anesthetic care have brightened, others remain in the dark ages.
Pediatric induction, for example, has remained unchanged since the early 20th century. But as the old adage goes: if it isn’t broken, don’t fix it. A standard mask induction works well enough and it’s easy: lay the child on the operating room table, place the anesthesia mask over his nose and mouth, turn on the oxygen-gas admixture, then watch as he gently drifts off to sleep. No needles. Simple. But easy? Well, not so fast.
Why Change Now?
Pediatric induction can be one of the most difficult techniques to master as well as the most stressful moment for a child undergoing surgery. More than 50% of children experience anxiety during the process. Crying, kicking, hitting and other forms of physical and verbal resistance to the noxious gasses often necessitate the need for physical restraint of the child, euphemistically referred to as brutane. A list of predictors for “noncompliant children” include younger age and shy temperament, but any child can decompensate once the anesthesia mask is placed. No amount of bubble gum flavoring can disguise the scent of Sevoflurane and, as far as distraction, there aren’t enough princess stickers, sing-along songs or videos to win over an inconsolable child.
That’s not to say all children react in this manner, but a high proportion are upset by the process of induction. Younger children suffer acute distress while children of all ages show signs of anticipatory distress. Children in need of frequent visits to the operating room (OR) experience even higher degrees of anxiety. The negative memory encodes with repeated exposure leading to exaggerated negative behaviors. Small cues, like the site of the anesthesia mask, elicit large consequences.
You Can’t Fool
A Veteran Of The Operating Room
Even If She’s only 4 Years Old
There's no fooling a veteran of the operating room, even if she's only four years old.
The effects of this bad experience last long after the moments it takes the child to fall asleep. When a child suffers anxiety at induction, she often develops a greater degree of postoperative emergence delirium. In the post-anesthesia recovery unit (PACU), these children exhibit crying fits and increased levels of pain. And it doesn’t end there. Post-discharge, parents report negative behaviors such as regression, bedwetting, nightmares, separation anxiety, temper tantrums and distrust of medical personnel. These stress-effects typically last two weeks for most children with some extending six months and, on rare occasions, a year.
Parents are also affected by the stress of induction. With the growing popularity of family-centered care, parental presence in the operating room during induction has morphed from a privilege to a standard. But contrary to popular belief, parental presence in the OR does not necessarily alleviate the child’s anxiety nor their own. Parents exhibit clinically significant signs of distress and those feelings can transfer from parent to child. Mom or dad sit on the sidelines, ever-watchful yet helpless as the child struggles against the anesthesia mask and well-meaning OR staff. The parent is told repeatedly the crying is “normal”, the process, “standard”. But does standard have to be accepted?
Alleviating Intraoperative Anxiety
To alleviate the intraoperative anxiety and negative postoperative behavior, a plethora of pharmacological modalities have been tried but with mixed success. At one time, midazolam was touted as the magic bullet. But the bullet missed the mark. In some children, oral midazolam causes a paradoxical effect. Instead of sedation, it elicits agitation, aggression, restlessness and self-injury making a bad situation worse.
Midazolam is also avoided as a routine order for more pragmatic reasons. Timing of this oral benzodiazepine makes it’s use difficult in the setting of a busy OR. Also, cooperation by the child is imperative. And an anxious child may refuse to drink it. Finally, in these days of shrinking medical dollars, oral sedation preoperatively may delay emergence from anesthesia and postoperative discharge thereby increasing operating costs.
On the other end of the spectrum, some nonpharmacological approaches have been shown to reduce perioperative stress. The use of presurgical educational pamphlets, preoperative visits, play therapy, music therapy and even doctors dressed as clowns have been shown to attenuate anxiety. Distraction is the key. Today, with the ever-increasing accessibility of tablets, cell phones and YouTube, distraction is only an app away. An internet search quickly retrieves a favorite cartoon, song, or video game making the ride back to the OR pleasant if not carefree.
However, as a child crosses the threshold into the cold and austere world called the operating room (with its intimidating machines, clanking medical instruments, and strangers), the electronics go down and the anxiety goes up. Once the child realizes the “pilot’s mask” doesn’t smell like bubblegum, playtime is over.
Or is it?
Why not continue the play in the operating room? Why not dedicate specific rooms for pediatrics? Have cartoon characters on the wall? Bright colors? Familiar music in the background?
Change is necessary but a change in operating room protocol and mindset is even more important than aesthetics. Once the child and parent enter the OR, full attention should turn to them: no counting of instruments and OR-talk. The child is the most important person in the room, so treat them with respect and dignity. Maintain eye contact. Speak to her. Give him choices whenever possible. Ask, “Would you like to sit up on the table or on mom’s (or dad’s) lap? Which finger do you want the finger-sticker on? Do you want to hold the mask?”
Then prepare for induction. Once the anesthesia circuit is primed with nitrous, allow the child to assist you if she chooses. Have her hold the mask to her face. If she resists, gently hold her hands at her side while your sing a song. Then slowly dial up the anesthetic gas.
Alternatively, try an anesthesia induction device. A number of mask-base distraction devices have been created over the years and one mask-free device is now under investigation. Mask-free? Why not? If science and technology can build a better robot to improve surgical outcomes, it can build a better device to improve induction.
In closing, it’s time to address this unfulfilled need. We must update the process of pediatric induction, bring it out of the dark ages and into the 21st century. New methods, innovative devices, and and endless list of intraoperative play are needed to relieve anxiety, avoid negative postoperative behavior changes and engender trust in the medical personnel. The operating room can and should be nurturing, comforting and fun. After all, the patient, parent and even practitioner deserve a positive experience.
Utilizing A Mask-Free Induction System
Instead of the scary, claustrophobic-feeling, foul-smelling anesthesia mask and dozens of distraction techniques that don’t work because they STILL use a mask, try PEDIA! The Pediatric Device for Induction of Anesthesia, Pedia Anesthesia Balloons, are the world’s first MASK-FREE anesthesia gas delivery system designed just for kids. The colorful balloons and whistling sounds of this anesthesia “toy” distracts, engages and engenders cooperation. Try it today. Visit PediaLLC.com or email contact@pediallc.com.
https://pediallc.com/wp-content/uploads/2015/02/desat-girl-m15.jpg850850dianemillerhttps://pediallc.com/wp-content/uploads/2021/02/PeDIA_header_1.pngdianemiller2021-08-18 17:22:112021-08-18 18:15:35Pediatric Anxiety During Induction of Anesthesia
Which is better: a mask-free anesthesia gas delivery system or “the old standard” mask induction? The ultimate goal is safety, of course, but providing a stellar experience in the operating room is a very close second. For children, that matters even more. You may want to know why we don’t just stick with the standard mask? If it ain’t broke, why fix it? Well, it is broken and has been for almost a century.
General Anesthesia for Children: Imagine you are a child in an operating room, surrounded by strangers in masks, strange machines and sounds. Then, these masked strangers hold your hands and feet still while they force a plastic mask on your face. It’s a little hard to breathe. Then comes the SMELL of anesthesia gases–ugh! You push away the mask, say no, cry, kick and try to get away. The more you fight, the harder they hold you down. It’s like a live horror movie. You’re trapped and no one–not even your parents–will help you. It’s the ultimate betrayal. You don’t remember falling asleep but you dream about this for weeks. You wet the bed, have nightmares and feel anxious. You then vow to never let them do this to you again. You no longer trust doctors and nurses.
As you can see, this negative experience causes more harm than good for a child. Even with distraction (iPhones, games…), nothing can get rid of the smell and feel of the mask. So PeDIA just got ride of the mask!
As far as parents are concerned, they worry about every aspect of their child’s anesthesia and surgery. Then, to see their child struggle causes much emotional turmoil and a feeling of helplessness. That does not equate to a good surgical experience from their point of view. The PeDIA device goes a long way to ease that fear: both the parent’s and the child’s.
Here’s What Parents Must Know About Their Child’s Anesthesia Care
If your child is undergoing anesthesia or surgery, do not hesitate to connect with an anesthesiology expert. They will discuss potential side effects, the child’s experience during anesthesia, and the recovery period. Ask them about the induction process: how, when and where; mask or no mask. It’s your right to ask as many questions as you can. Doctors and nurses know medicine but only YOU know your child.
If PeDIA seems like a great alternative to the mask, as your surgeon or anesthesia team about the Pediatric Device for Induction of Anesthesia–Pedia Anesthesia Balloon the only mask-free anesthesia gas delivery system available on the market! https://www.PediaLLC.com
Anesthesia Medical Devices: How Anesthesiologist’s Care will Make Your Child
The anesthesiologist works with you and your surgeon to deliver safe, effective care and to make sure the entire process is a success. Let PeDIA help the doctors and nurses make it less traumatic and, perhaps, even fun with our colorful, whistling balloons.
A few more things. Your child must be NPO. That means, they should not eat or drink anything before surgery. This is to protect your child from harm during induction. Check with your anesthesiologist to see how long they should be without food or drink. Before surgery, during your anesthesia interview, tell your anesthesiologist about your child’s medical history. If your child has a favorite toy, they may let him or her bring it back into the operating room. If you will accompany your child for induction, you may be asked to wear a special coverup and surgical booties over your shoes as well as a surgical hat. In the operating room, the team may ask you to stand near the operating room table next to your child or sit in a chair and hold your child in your lap.
Before Surgery, Make Sure to Have the Talk with Your Child:
This doesn’t have to be a serious talk. Your child may have questions so answer them according to their understanding. Let them know the doctors and nurses will be there to take care of them. In the preoperative room, address any questions you or your child have. It will bring assurance to your child, and they might feel less anxious and worried.
Final Words
Join the PeDIA Movement. Switch from the archaic mask-based anesthesia induction to the 21st century PeDIA Induction.
https://www.PediaLLC.com or email us directly at contact@pediall.com
https://pediallc.com/wp-content/uploads/2021/08/Playful-Green-Virtual-Classroom.png10801920dianemillerhttps://pediallc.com/wp-content/uploads/2021/02/PeDIA_header_1.pngdianemiller2021-08-11 12:27:262025-06-26 19:29:08The Revolutionary PeDIA Induction vs “Standard” Mask-Based Induction